

How nurses can support patients undergoing knee replacement surgery, including optimising care pre-, peri- and post-operatively to improve health outcomes
Abstract
Knee replacement (arthroplasty) is a common procedure used to improve the function of the knee. This article, the second in a series of three on the knee joint, considers how nurses, as part of the multidisciplinary team, can support patients across the surgical journey, including optimising health before surgery and in the peri- and post-operative stages of care. It shows how providing clear, timely information is an essential part of shared decision making to enable the patient to take an active role in their care.
Citation: Walker J, Dimcea G (2025) How to optimise care of a patient undergoing knee replacement surgery. Nursing Times [online], 121; 3.
Author: Jennie Walker is principal lecturer and Gruia Dimcea is senior lecturer, Institute of Health and Allied Professions, Nottingham Trent University.
- This article has been double-blind peer reviewed
- Scroll down to read the article or download a print-friendly PDF here (if the PDF fails to fully download please try again using a different browser)
- Click here to see other articles in this series
Introduction
A knee replacement (arthroplasty) is a surgical procedure to replace damaged parts of the knee. It is commonly used to manage pain and reduced function caused by conditions such as osteoarthritis, inflammatory arthritis (for example, rheumatoid arthritis) and osteonecrosis (Granicher et al, 2022). Knee trauma or fractures may also require surgical management with an arthroplasty to preserve function.
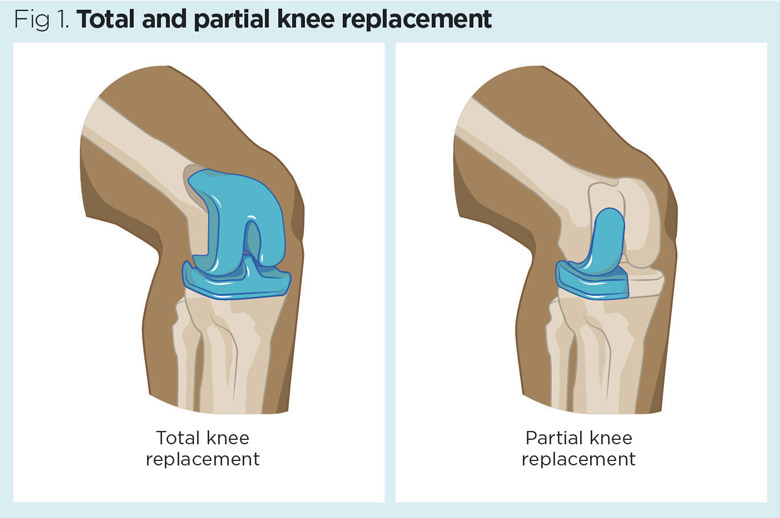
Depending on the extent of damage, some or all the knee surfaces may be replaced. These procedures are known as partial (or hemi) and total knee arthroplasty (Fig 1). Each year more than 90,000 total knee replacements are performed in the UK (Anderson et al, 2021). Evans et al (2019) estimate that 70% of partial knee replacements last 25 years and 82% of total knee replacements last 25 years.
After the decision has been made to schedule a patient for a knee replacement, there may be a considerable waiting period. While waiting, patients can experience functional limitations, severe pain and psychological distress (Anderson et al, 2021), so their overall condition may deteriorate.
Poor physical and mental health status are associated with poorer post-operative recovery (De Klerk et al, 2023). Lower levels of pre-operative functional capacity are associated with higher morbidity and mortality, reduced quality of life and loss of independence (Carli and Balindi, 2021).
Prehabilitation is a proactive approach to enhance the patient’s physical and mental readiness for surgery and reduce the impact of the procedure (Gillis et al, 2022). Pre-operative optimisation of the physical functional capacity focuses on physical, nutritional and psychological elements (Carli and Balindi, 2021).
Prehabilitation
Pre-operative exercise has been shown to have a positive effective on post-operative knee function (Chen et al, 2018), length of hospital stay (De Klerk et al, 2023) and health-related quality of life (Anderson et al, 2021). Enhancement of physical fitness should aim to increase lean muscle mass and enhance aerobic capacity (Durrand et al, 2019).
Major surgery, such as a knee replacement, can trigger a catabolic state; this is a stress response in which energy demands exceed the supply (Gillis et al, 2022). Patients lacking the necessary reserves to respond to this demand experience statistically significantly worse outcomes post-operatively (Durrand et al, 2019). While pre-operative healthy eating advice is helpful, a focused nutritional assessment is required and the Malnutrition Universal Screening Tool (MUST) is recommended to assess for malnutrition (Gillis and Wischmeyer, 2019). Where a deficit is identified, a targeted approach is needed to optimise nutritional status and ensure sufficient intake of daily nutrients, including a daily protein consumption of 1.5-2.0g per kg of body weight (Gillis and Wischmeyer, 2019).
Frail older patients will have limited reserves to manage the impact of surgery (Carli and Balindi, 2021). This increases their risk of post-operative complications and prolonged hospitalisation (Carli and Balindi, 2021). The well-established Timed Up and Go (TUG) test can be used to measure functional capacity, including timing how long it takes to stand up from a chair, walk 3m, turn and return to sitting in the chair; where this takes 15 seconds or longer, it is considered a slow response and a predictor of increased risk of post-operative complications and mortality at one year (Robinson et al, 2013). Addressing frailty pre-operatively may require specialist geriatric services and a multifactorial approach to optimising the patient’s condition before surgery (National Institute for Health and Care Excellence (NICE), 2020a).
Smoking tobacco is associated with significantly higher risks of post-operative complications, such as infection and delayed wound healing (World Health Organization (WHO), 2020). Improving lung function prior to surgery will help improve oxygenation and reduce the risk of atelectasis (collapse of the lung alveoli). Smoking status should be established and smoking cessation advice given where necessary. It is recommended patients stop smoking at least four weeks before surgery (Wainright et al, 2020). Use of pre-operative inspiratory muscle training may also be considered to reduce post-operative pulmonary complications, such as chest infections (Durrand et al, 2019).
Individuals who drink above the recommended alcohol threshold (14 units per week) are also at increased risk of complications, therefore, interventions to reduce alcohol consumption will lower the incidence of post-operative complications (Egholm et al, 2018). Rotevatn et al (2017) have reported that the risk of venous thromboembolism (VTE), infection and cardiovascular disease are lower in those who abstain from alcohol.
Psychosocial states
Patients with severe pre-operative anxiety, depression or stress experience worse surgical outcomes (Gillis et al, 2022). This may be due to the heightened stress response reducing immune function (Manou-Stathopoulou et al, 2019), some anxious patients needing more anaesthesia (Gillies et al, 2022), or individuals with depression being less physically active and having lower functional reserves (Barrett-Bernstein et al, 2019). It is, therefore, important to assess an individual’s psychological wellbeing and offer strategies to reduce distress. Psychological preparation can also have beneficial effects on post-operative pain and length of hospital admission (Powell et al, 2016). As well as emotional support, interventions to promote self-efficacy may include deep breathing, relaxation techniques and guided imagery (Gilles et al, 2022).
Pre-operative assessment
Individuals undergoing elective surgery are required to attend a pre-operative assessment to identify health conditions that may lead to complications during the peri- or post-operative period. Pre-operative assessments consider comorbidities, functional capacity and age-related features, such as cognitive impairment, sarcopenia, polypharmacy and malnutrition to inform risk assessment (Carli and Balindi, 2021).
Home circumstances are another important part of the pre-operative assessment, as this can inform discharge planning and facilitate early preparation to allow prompt discharge from hospital. A holistic approach to patient assessment is required, including consideration of the home environment (for example, access to the house, stairs and height of chairs), social support networks and social roles and responsibilities that may be impacted by the surgery.
All patients undergoing major or complex surgery, such as knee replacement, will require a pre-operative full blood count (NICE, 2016). Individuals who may be at risk of acute kidney injury, or with systemic disease, will require assessment of kidney function (NICE, 2016). Assessment of haemostasis is not routinely required but may be reviewed in people with chronic liver disease or who take anticoagulants (NICE, 2016). Electrocardiograms (ECG) may be considered for healthy individuals, aged over 65 years if there is no previous ECG documented in the past 12 months, and ECG should be performed routinely where the person has systemic disease (NICE, 2016). To reduce the risk of surgical site infection, an infection screen may be completed at the pre-operative assessment to assess for MRSA or urinary tract infection.
Sickle cell testing is not routinely required before surgery, but where the patient is known to have sickle cell disease and is under the care of a specialist, liaison with the sickle cell team prior to surgery is recommended (NICE, 2016). Women of childbearing age should be asked if there is any possibility of them being pregnant, whereupon a pregnancy test should be considered and the woman made aware of the risk of the anaesthetic and surgical procedure to the unborn child (NICE, 2016).
Pre-operative information
Pre-operative information helps set realistic expectations (Anderson et al, 2021). It enables patients to anticipate what is to come and to prepare, which reduces anxiety and fear (Edwards et al, 2017). Box 1 shows key information to give to patients.
Box 1. Patient information to be given pre-operatively
- What to expect during the pre-, peri- and post-operative phases of care
- How to prepare for surgery
- Post-operative pain management
- Wound care
- Return to usual activities
Source: National Institute for Health and Care Excellence (2020b)
Timely information enables informed decision making, as patients can learn about the risks and benefits of certain actions, such as smoking and having a healthy diet. It is not just the responsibility of the surgical team to inform patients about lifestyle modifications. The Making Every Contact Count approach facilitates cross sector working and wide-reaching support to optimise health (Durrand et al, 2019).
The timing and format of information are important. Pre-operative anxiety peaks in the immediate period before surgery, so having information prior to this allows patients time to prepare. Where possible, verbal information should be reinforced with written information, which also allows information to be revisited or shared with friends and family. An early study by Anderson et al (1979) observed that individuals only remember 40% of verbal information, but this increases to approximately 70% with written information. Use of information leaflets, such as those by the Royal College of Surgeons can be used to supplement verbal information and offer a clear standardised approach.
Clear precise information is needed to guide patients on what to do and how to do it (Durrand et al, 2019). Effective pre-operative education can reduce the length of hospital stay (McDonald et al, 2014) and has also been reported to increase discharge home and reduce readmissions to hospital (Edwards et al, 2017). Earlier discharges may be partly due to patients being more informed about post-operative care, enabling them to practice techniques pre-operatively, such as getting out of bed or focused exercises. Knowing what to expect also makes it easier for patients to proactively prepare for discharge prior to admission; for example, by pre-preparing and freezing meals, stocking food cupboards and arranging for someone to collect milk and bread on the day of discharge.
Pre-operative information increases patient satisfaction as patients understand the recovery process and are empowered to actively participate in their own care (Edwards et al, 2017). Clear information can help with pain management, by letting patients know what to expect and how to effectively use pain management techniques and coping strategies (Edwards et al, 2017). It can also advise on possible complications, how to reduce the risk of occurrence and what to look out for. This increases patient vigilance and enables early identification of complications.
“Patients who suffer with severe pre-operative anxiety, depression or stress experience worse surgical outcomes”
Perioperative care
Patients undergoing elective surgery are usually admitted on the day of surgery and, in some cases, may be booked for a day case procedure (Dey et al, 2021). Therefore, clear instructions need to be provided pre-admission to allow patients to prepare for their surgery. Fasting is required to reduce the risk of pulmonary aspiration (Smith et al, 2011). Patients should be starved of food six hours prior to surgery and permitted clear fluids up to two hours before surgery (Smith et al, 2011). Clear fluids include water, tea or coffee without milk and fruit juice (without pulp) (NICE, 2020a). Limiting fasting periods before surgery can minimise the stress response to surgery and help maintain homeostasis (Gillis et al, 2022). Likewise, drinking clear fluids can reduce post-operative headaches and nausea and vomiting (NICE, 2020a).
To help reduce the risk of surgical site infection, patients should shower or bathe before surgery (NICE, 2020c). Prior to the patient being transferred to the anaesthetic room (and before pre-medication is taken) the limb should be marked to ensure the correct site is operated on (Centre for Perioperative Care, no date). The WHO surgical safety checklist (WHO, 2009) is designed to improve the safety of surgical care and eliminate preventable events (never events) (NICE, 2020a). It has three key checkpoints:
- Before the induction of anaesthesia;
- Before skin incision;
- Before the patient leaves the operating theatre.
Individuals undergoing primary elective knee replacements can choose whether to have surgery with regional or general anaesthesia (NICE, 2020b). This is guided by medical conditions and risk factors, but patient choice is also important. Local infiltration analgesia is recommended, regardless of the regional or general anaesthetic (NICE, 2020b). Prior to incision, the surgical site is prepared by the operating team with alcoholic chlorhexidine (NICE, 2020c). Antibiotic prophylaxis should also be used to reduce risk of wound infection (NICE 2020c; Wainwright et al, 2020).
The surgical technique will vary according to the type of implant and surgeon preference but involves removing the damaged areas of the joint (cartilage and bone) and replacing it with the implant. As this type of surgery can cause significant blood loss, tranexamic acid may be used during surgery to reduce blood loss and the need for subsequent blood transfusion (NICE, 2020b; Wainwright et al, 2020).
Post-operative care
Following surgery, patients are transferred to a post-operative assessment unit for close monitoring (NICE, 2020a). Regular assessment of blood pressure, pulse, respiratory rate and oxygen saturation levels are required. Use of early warning score systems help practitioners identify risks for deterioration and advise on possible routes for escalation and action (Royal College of Physicians, 2017).
Normothermia (normal body temperature) should be maintained where possible, as this promotes healing and reduces the risk of surgical site infection (NICE, 2020c). As well as assessment of vital signs, close observation of the fluid balance is required, such as intravenous fluids, oral intake and output from urine or drains. Routine use of catheters is not recommended. Where catheters have been inserted during surgery, they should be removed as soon as possible, ideally within 24 hours (Wainwright et al, 2020).
Post-operative nausea and vomiting (PONV) is an unpleasant side-effect, which can cause delayed hospital discharge (Wainwright et al, 2020). Those most at risk are females, non-smokers, and those with a previous history of PONV or motion sickness (Wainwright et al, 2020). A prophylactic antiemetic may be given during surgery, but further treatment may be required with other antiemetics if PONV continues to be problematic (Wainwright et al, 2020).
Dressings are applied in theatre to cover and protect the surgical site and reduce the risk of contamination. Dressings should be checked regularly in the immediate post-operative period to assess for bleeding or excessive leakage. The WHO (2018) recommends that dressings remain undisturbed for at least 48 hours, unless there is excessive leakage, which requires a dressing change. Where this is required, an aseptic non-touch technique must be used (NICE, 2020c). Patients may safely shower after 48 hours (NICE, 2020c).
Nurses have an important role in observing for infection to ensure prompt identification and management. Local signs and symptoms of surgical site infection include erythema (reddening of the skin), increased localised temperature and purulent drainage from the wound. Systemic signs include pyrexia (fever), raised white cell count and loss of appetite (NICE, 2020c). Where infection is suspected, wound swabs and blood cultures may be required to identify the microorganisms and inform prescribing of targeted antimicrobial therapy.
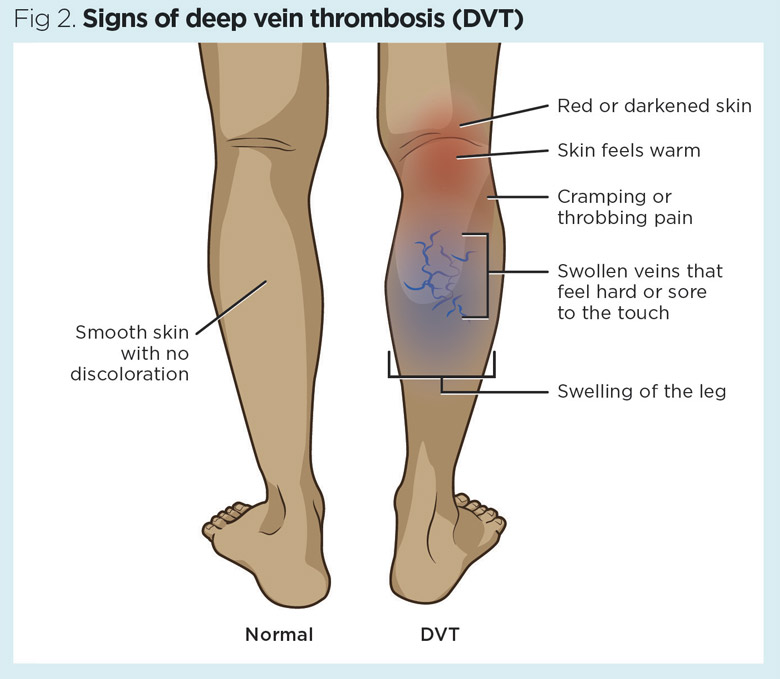
Patients undergoing knee arthroplasty surgery are at risk of DVT and pulmonary embolism (PE) and should, therefore, be encouraged to mobilise as soon as possible after surgery (Wainwright et al, 2020). VTE risk should be assessed and VTE prophylaxis is required where the risk of VTE outweighs risk of bleeding (NICE, 2019). Signs of deep vein thrombosis include swelling and pain in the leg, which is warm to touch and may be darker or red in colour (Fig 2).
Pain management
Acute pain following surgery is common and up to 25% of patients go on to develop chronic pain following their recovery if the acute stage is not managed appropriately (Wylde et al, 2022). The main pain mechanisms following surgery relate to local inflammation and nerve sensitisation, with pain increasing in the first two days post-op, then subsiding after day three and plateauing after 45 days post-op (Lebleu et al, 2023).
Effective pain assessment and management are vital to ensure patient comfort and to optimise recovery. Pain should be assessed regularly using a self-reporting pain assessment tool, such as a numerical rating scale, as this allows patients to rate their level of pain. It is also important to consider the quality and character of the pain, so that pain management can be personalised. Recent reviews have highlighted the importance of managing acute pain effectively with intra-operative pharmacological strategies (a single adductor nerve block, local-infiltration-anaesthetic and a dose of intravenous dexamethasone) and multi-modal analgesia post-operatively with paracetamol and non-steroidal anti-inflammatory drugs (NSAIDs) (Lavand’homme et al, 2022). NICE (2020d) recommends oral paracetamol, NSAIDs and opioids for immediate post-operative pain, although patient-controlled-analgesia or continuous epidural may be used for managing severe pain in the immediate post-operative period. Intravenous ketamine and oral gabapentin may also be used if the pain is severe (NICE, 2020d).
Non-pharmacological strategies, such as guided imagery, relaxation techniques and music therapy can be used as part of a holistic approach towards pain management. The Support and Treatment After Replacement (STAR) care pathway has evolved into an established and bespoke pain management intervention for patients following knee replacement (Wylde et al, 2022) (Box 2).
Box 2. STAR care pathway
The Support and Treatment After Replacement (STAR) intervention is a care pathway for patients who are at risk of developing chronic pain following knee replacement surgery. The initial trial started with a post-operative three-month assessment and targeted treatment pathway, with referrals and telephone follow-up over 12 months (Wylde et al, 2022). The initial assessment consisted of a physical examination, assessment of pain characteristics and severity, and onward referrals to physiotherapy, occupational therapy, orthopaedics or community pain clinics as required (Wylde et al, 2022). A follow-up study by Bertram et al (2023) compared, not only the initial data, but ongoing recovery and outcomes. Despite significant participant attrition concerns, the bespoke intervention succeeded in reducing pain severity, improving quality of life and reducing hospital admissions and overall NHS cost (Bertram et al, 2023).
Physiotherapy
Patients should receive a proactive multi-disciplinary team-based, active post-operative rehabilitation plan before discharge (NICE, 2022b). Best practice guidance from the Getting it Right the First Time (GIRFT) team on ambulatory care for elective hip and knee patients has led to recommendations for early mobilisation, a return to normal activities and getting up and dressed as soon as possible (GIRFT, 2022).
Physiotherapy needs to be patient-centred, starting with passive and active mobilisation of the limb, before progressing onto mobility, balance and strength exercises – with a focus on motor function, strength and balance retraining (Jette et al, 2020). Exercise, such as hydrotherapy, as well as cryotherapy (cold therapy) and manual therapy have shown improvements (Argut et al, 2020; Henderson et al, 2017). Novel techniques, such as hybrid-assistive-limb training (a wearable robot device that can assist voluntary knee joint motion), are also under investigation, with some promising results compared with conventional rehabilitation, but are not currently recommended over an educational, goal-orientated and exercise-based approach (Yoo et al, 2022).
While surgery may be completed successfully and post-operative complications avoided, recovery can be prolonged and is influenced by pre-operative levels of activity and the presence of comorbidities. Discussions around ongoing recovery and a return to usual activity should be started in the pre-operative phase to give the patient realistic expectations. Use of patient-reported outcome measures can help give a personalised approach to monitoring progress and confidence with performing daily living activities.
Conclusion
Knee replacements are a common orthopaedic procedure to improve knee function. Nurses have a central role in the multidisciplinary team to support patients across the different phases of care in both acute and community settings. Providing clear and timely information is essential to empower patients to actively participate in their care and understand what to expect during and after surgery. Prehabilitation and optimising physical and mental health are key to ensuring patients are in the best possible condition for surgery. This helps prepare them for the peri- and post-operative phases, and enables them to take proactive measures to minimise the risk of complications and expediate their return to usual activity.
Key points
- Knee replacements are increasingly being performed as day-case procedures
- Prehabilitation can optimise a patient’s condition prior to surgery to improve outcomes
- Pre-operative information can help reduce anxiety and enable patients to actively participate in their care
- Early mobilisation after surgery supports patients to return to usual activities of daily living, reducing the risk of complications
- ‘Making every contact count’ is important to support patients in the pre- and post-operative phases
Anderson J et al (1979) Patient information recall in a rheumatology clinic. Rheumatology Rehabilitation; 18: 1, 18–22.
Argut SK et al (2021) The combination of exercise and manual therapy versus exercise alone in total knee arthroplasty rehabilitation: A Randomized Controlled Clinical Trial. Physical Medicine and Rehabilitation; 13: 10, 1069-1078.
Barrett-Bernstein M et al (2019) Depression and functional status in colorectal cancer patients awaiting surgery: impact of a multimodal prehabilitation program. Health Psychology; 38: 10, 900-909.
Bertram W et al (2023) The STAR care pathway for patients with chronic pain after total knee replacement: four-year follow-up of a randomised controlled trial. BMC Musculoskeletal Disordorders; 24: 972 (2023).
Carli F, Baldini G (2021) From preoperative assessment to preoperative optimization of frail older patients. European Journal of Surgical Oncology; 47: 3, 519-523.
Centre for Perioperative Care (no date) The National Safety Standards for Invasive Procedures (NatSSIPs) 2: Consent, Procedural Verification and Site Marking. CPOC
Chen H et al (2018) Is it necessary to perform prehabilitation exercise for patients undergoing total knee arthroplasty: meta-analysis of randomized controlled trials. The Physician and Sports Medicine; 46: 1, 36-43.
De Klerk T et al (2023) Effects of home-based prehabilitation on pre-and postoperative outcomes following total hip and knee arthroplasty: a systematic review and meta-analysis. Bone & Joint Open; 4: 5, 315-328.
Dey S et al (2021) The safety and efficacy of day-case total joint arthroplasty. The Annals of The Royal College of Surgeons of England; 103: 9, 638-644.
Durrand J et al (2019) Prehabilitation. Clinical Medicine; 19: 6, 458–64.
Edwards PK et al (2017) Preoperative education for hip and knee replacement: never stop learning. Current Reviews in Musculoskeletal Medicine; 10: 3, 356–364.
Egholm JWM et al (2018) Perioperative alcohol cessation intervention for postoperative complications. Cochrane Database of Systematic Reviews; 11: CD008343.
Evans J et al (2019) How long does a knee replacement last? A systematic review and meta-analysis of case series and national registry reports with more than 15 years of follow-up. Lancet; 393: 10172, 655-663.
Getting it Right the First Time (2022) Total & Uni Primary Knee Replacement Recommendations. Online. gettingitrightthefirsttime.co.uk, November (accessed 21 January 2025)
Gillis C et al (2022) Prehabilitation, enhanced recovery after surgery, or both? A narrative review. British Journal of Anaesthesia; 128: 3, 434-448.
Gillis C, Wischmeyer P (2019) Pre‐operative nutrition and the elective surgical patient: why, how and what? Anaesthesia; 74: S1, 27-35.
Gränicher P et al (2022) Prehabilitation improves knee functioning before and within the first year after total knee arthroplasty: A systematic review with meta-analysis. Journal of Orthopaedic & Sports Physical Therapy; 52: 11, 709-725.
Henderson KG et al (2018) Active physiotherapy interventions following total knee arthroplasty in the hospital and inpatient rehabilitation settings: a systematic review and meta-analysis. Physiotherapy; 104: 1, 25–35.
Jette DU et al, American Physical Therapy Association (2020) Physical therapist management of total knee arthroplasty. Physical Therapy; 100: 9, 1603–1631.
Lavand’homme PM et al (2022) Pain management after total knee arthroplasty. European Journal of Anaesthesiology; 39: 9, 743–757.
Lebleu J et al (2023) Severe postoperative pain in total knee arthroplasty patients: risk factors, insights and implications for pain management via a digital health approach. Journal of Clinical Medicine; 12: 24, 7695.
McDonald S et al (2014) Preoperative education for hip or knee replacement. Cochrane Database Systematic Reviews; 5:CD003526.
Manou-Stathopoulou V et al (2019) Redefining the perioperative stress response: a narrative review. British Journal of Anaesthesia; 123: 5, 570-583.
National Institute for Health and Care Excellence (2020a) Perioperative Care in Adults. NICE.
National Institute for Health and Care Excellence (2020b) Joint Replacement (Primary): Hip, Knee and Shoulder. NICE.
National Institute for Health and Care Excellence (2020c) Surgical Site Infections: Prevention and Treatment. NICE.
National Institute for Health and Care Excellence (2020d) Perioperative Care in Adults – Managing Pain. NICE.
National Institute for Health and Care Excellence (2019) Venous Thromboembolism in Over 16s: Reducing the Risk of Hospital-Acquired Deep Vein Thrombosis or Pulmonary Embolism. NICE.
National Institute for Health and Care Excellence (2016) Routine Pre-operative Tests for Elective Surgery. NICE.
Powell R et al (2016) Psychological preparation and postoperative outcomes for adults undergoing surgery under general anaesthesia. Cochrane Database Systematic Reviews; 5:CD008646.
Robinson TN et al (2013) Slower walking speed forecasts increased postoperative morbidity and 1-year mortality across surgical specialties. Annals of Surgery; 258: 4, 582-588.
Rotevatn TA et al (2017) Alcohol consumption and the risk of postoperative mortality and morbidity after primary hip or knee arthroplasty – a register-based cohort study. PLoS One; 12: 3:e0173083.
Royal College of Physicians (2017) National Early Warning Score (NEWS) 2: Standardising the Assessment of Acute-Illness Severity in the NHS. RCP.
Smith I et al (2011) Perioperative fasting in adults and children: guidelines from the European Society of Anaesthesiology. European Journal of Anaesthesiology, 28; 8, 556-569.
Wainwright T et al (2020) Consensus statement for perioperative care in total hip replacement and total knee replacement surgery: Enhanced Recovery After Surgery (ERAS) Society recommendations. Acta Orthopaedica; 91:1, 3-19.
World Health Organization (2020) Smoking greatly increases the risk of complications after surgery, who.int, 20 January (accessed 21 January 2025)
World Health Organization (2018) Global Guidance for the Prevention of Surgical Site Infection. WHO.
World Health Organization (2009) Surgical Safety Checklist. WHO.
Wylde V et al (2022) The STAR care pathway for patients with pain at 3 months after total knee replacement: a multicentre, pragmatic, randomised, controlled trial; The Lancet Rheumatology; 4: 3, e188–e197.
Yoo JI et al (2022) Robot-assisted rehabilitation for total knee or hip replacement surgery patients: A systematic review and meta-analysis. Medicine; 101: 40, e30852.
Help Nursing Times improve
Help us better understand how you use our clinical articles, what you think about them and how you would improve them. Please complete our short survey.
link